Health Care In The United States - Us Healthcare Budget
Health care in the United States is provided by many distinct organizations. Health care facilities are largely owned and operated by private sector businesses. 58% of US community hospitals are non-profit, 21% are government owned, and 21% are for-profit. According to the World Health Organization (WHO), the United States spent more on health care per capita ($8,608), and more on health care as percentage of its GDP (17.2%), than any other nation in 2011.
60â€"65% of healthcare provision and spending comes from programs such as Medicare, Medicaid, the Children's Health Insurance Program, and the Veterans Health Administration. Most of the population under 67 is insured by their or a family member's employer, some buy health insurance on their own, and the remainder are uninsured. Health insurance for public sector employees is primarily provided by the government.
The United States life expectancy of 78.4 years at birth, up from 75.2 years in 1990, ranks it 50th among 221 nations, and 27th out of the 34 industrialized OECD countries, down from 20th in 1990. Of 17 high-income countries studied by the National Institutes of Health in 2013, the United States had the highest or near-highest prevalence of obesity, car accidents, infant mortality, heart and lung disease, sexually transmitted infections, adolescent pregnancies, injuries, and homicides. On average, a U.S. male can be expected to live almost four fewer years than those in the top-ranked country, though notably Americans aged 75 live longer than those who reach that age in other developed nations.
A comprehensive 2007 study by European doctors found the five-year cancer survival rate was significantly higher in the U.S. than in all 21 European nations studied, 66.3% for men versus the European mean of 47.3% and 62.9% versus 52.8% for women. Americans undergo cancer screenings at significantly higher rates than people in other developed countries, and access MRI and CT scans at the highest rate of any OECD nation. People in the U.S. diagnosed with high cholesterol or hypertension access pharmaceutical treatments at higher rates than those diagnosed in other developed nations, and are more likely to successfully control the conditions. Diabetics are more likely to receive treatment and meet treatment targets in the U.S. than in Canada, England, or Scotland. A study showed that the U.S., Japan, and France recorded the highest survival rates among 31 nations for four types of cancer.
America is a global leader in medical innovation. The US solely developed or contributed significantly to 9 of the top 10 most important medical innovations since 1975 as ranked by a 2001 poll of physicians, while the EU and Switzerland together contributed to five. Since 1966, Americans have received more Nobel Prizes in Medicine than the rest of the world combined. From 1989 to 2002, four times more money was invested in private biotechnology companies in America than in Europe. The United States also has the most advanced hospitals in the world.
Gallup recorded that the uninsured rate among U.S. adults was 11.9% for the first quarter of 2015, continuing the decline of the uninsured rate outset by the Affordable Care Act. A 2004 Institute of Medicine (IOM) report said: "The United States is among the few industrialized nations in the world that does not guarantee access to health care for its population." A 2004 OECD report said: "With the exception of Mexico, Turkey, and the United States, all OECD countries had achieved universal or near-universal (at least 98.4% insured) coverage of their populations by 1990." Recent evidence demonstrates that lack of health insurance causes some 45,000 to 48,000 unnecessary deaths every year in the United States. In 2007, 62.1% of filers for bankruptcies claimed high medical expenses. A 2013 study found that about 25% of all senior citizens declare bankruptcy due to medical expenses, and 43% are forced to mortgage or sell their primary residence.
On March 23, 2010, the Patient Protection and Affordable Care Act (PPACA) became law, providing for major changes in health insurance. The medical system will be forced to change normal procedures. They will be required to prepare for upcoming programs to meet federal regulations. The constitutionality of the law, as well as its impact on insurance coverage, insurance quality, insurance premiums, medical quality, and the economy are subjects of ongoing debate.
History
Puerto Rican protesters call for equal health care budget from US
Statistics
Health care facilities are largely owned and operated by private sector businesses. Health insurance for public sector employees is primarily provided by the government. 60â€"65% of healthcare provision and spending comes from programs such as Medicare, Medicaid, TRICARE, the Children's Health Insurance Program, and the Veterans Health Administration. Most of the population under 65 is insured by their, or a family member's employer. Some buy health insurance on their own, and the remainder are uninsured.
Of 17 high-income countries studied by the National Institutes of Health in 2013, the United States was at or near the top in infant mortality, heart and lung disease, sexually transmitted infections, adolescent pregnancies, injuries, homicides, and rates of disability. Together, such issues place the U.S. at the bottom of the list for life expectancy. On average, a U.S. male can be expected to live almost four fewer years than those in the top-ranked country.
A study by the National Institutes of Health reported that the lifetime per capita expenditure at birth, using year 2000 dollars, showed a large difference between health care costs of females ($361,192) and males ($268,679). A large portion of this cost difference is in the shorter lifespan of men, but even after adjustment for age (assume men live as long as women), there still is a 20% difference in lifetime health care expenditures.
There is evidence, however, that a large proportion of health outcomes and early mortality can be attributed to other factors. As a study by the National Research Council concluded, more than half the men who die before 50 die due to murder (19%), traffic accidents (18%), and other accidents (16%). For women the percentages are different. 53% of women who die before 50 die due to disease, whereas 38% die due to accidents, homicide, and suicide. However maternal deaths related to childbirth have increased. In 2013 18.5 mothers died for every 100,000 births. In 1987 the mortality rate was 7.2 per 100,000. The American rate is now more than double the maternal mortality rate in Saudi Arabia and Canada, and more than triple the rate in the United Kingdom.
A study by the Agency for Healthcare Research and Quality (AHRQ) found that there were 38.6 million hospital stays in the U.S. in 2011, an 11 percent increase since 1997. Since the population also grew during this period, the hospitalization rate remained stable at approximately 1,200 stays per 10,000 population.
The U.S. Census Bureau reported that 49.9 million residents, 16.3% of the population, were uninsured in 2010 (up from 49.0 million residents, 16.1% of the population, in 2009). According to the World Health Organization (WHO), the United States spent more on health care per capita ($7,146), and more on health care as percentage of its GDP (15.2%), than any other nation in 2008. The United States had the fourth highest level of government health care spending per capita ($3,426), behind three countries with higher levels of GDP per capita: Monaco, Luxembourg, and Norway. A 2001 study in five states found that medical debt contributed to 46.2% of all personal bankruptcies and in 2007, 62.1% of filers for bankruptcies claimed high medical expenses. Since then, health costs and the numbers of uninsured and underinsured have increased. A 2013 study found that about 25% of all senior citizens declare bankruptcy due to medical expenses.
Active debate about health care reform in the United States concerns questions of a right to health care, access, fairness, efficiency, cost, choice, value, and quality. Some have argued that the system does not deliver equivalent value for the money spent. The U.S. pays twice as much as Canada yet lags behind other wealthy nations in such measures as infant mortality and life expectancy. Currently, the U.S. has a higher infant mortality rate than most of the world's industrialized nations. In the United States life expectancy is 42nd in the world, after some other industrialized nations, lagging the other nations of the G5 (Japan, France, Germany, U.K., U.S.) and just after Chile (35th) and Cuba (37th).
Life expectancy at birth in the U.S., 78.49, is 50th in the world, below most developed nations and some developing nations. Monaco is first with 89.68. Chad is last with 48.69. With 72.4% Americans of European ancestry, life expectancy is below the average life expectancy for the European Union. The World Health Organization (WHO), in 2000, ranked the U.S. health care system as the highest in cost, first in responsiveness, 37th in overall performance, and 72nd by overall level of health (among 191 member nations included in the study). In 2008 the Commonwealth Fund, an advocacy group seeking greater government involvement in US healthcare, then led by former Carter administration official Karen Davis, ranked the United States last in the quality of health care among similar countries, and notes U.S. care costs the most.
United States ranks close to the bottom compared to other industrialized countries on several important health issues affecting mortality: low birth weight and infant mortality, injuries and murder, teen pregnancy and STDs, HIV and AIDS, deaths resulting from drug overdoses, obesity and diabetes, heart disease, COPD, and general disability.
A 2004 Institute of Medicine (IOM) report said: "The United States is among the few industrialized nations in the world that does not guarantee access to health care for its population." A 2004 OECD report said: "With the exception of Mexico, Turkey, and the United States, all OECD countries had achieved universal or near-universal (at least 98.4% insured) coverage of their populations by 1990." The 2004 IOM report observed "lack of health insurance causes roughly 18,000 unnecessary deaths every year in the United States", while a 2009 Harvard study conducted by co-founders of Physicians for a National Health Program, a pro-single payer advocacy group, estimated that 44,800 excess deaths occurred annually due to lack of health insurance. The group's methodology has been criticized by economist John C. Goodman for not looking at cause of death or tracking insurance status changes over time, including the time of death.
A 2009 study by former Clinton policy adviser Richard Kronick found no increased mortality from being uninsured after certain risk factors were controlled for, and specifically criticized the methodology used by IOM.
On March 23, 2010, the Patient Protection and Affordable Care Act (PPACA) became law, providing for major changes in health insurance.
Providers
Health care providers in the U.S. encompass individual health care personnel, health care facilities and medical products.

Facilities
In the U.S., ownership of the health care system is mainly in private hands, though federal, state, county, and city governments also own certain facilities.
The non-profit hospitals share of total hospital capacity has remained relatively stable (about 70%) for decades. There are also privately owned for-profit hospitals as well as government hospitals in some locations, mainly owned by county and city governments. The Hill-Burton Act was passed in 1946, which provided federal funding for hospitals in exchange for treating poor patients.
There is no nationwide system of government-owned medical facilities open to the general public but there are local government-owned medical facilities open to the general public. The U.S. Department of Defense operates field hospitals as well as permanent hospitals via the Military Health System to provide military-funded care to active military personnel.
The federal Veterans Health Administration operates VA hospitals open only to veterans, though veterans who seek medical care for conditions they did not receive while serving in the military are charged for services. The Indian Health Service (IHS) operates facilities open only to Native Americans from recognized tribes. These facilities, plus tribal facilities and privately contracted services funded by IHS to increase system capacity and capabilities, provide medical care to tribespeople beyond what can be paid for by any private insurance or other government programs.
Hospitals provide some outpatient care in their emergency rooms and specialty clinics, but primarily exist to provide inpatient care. Hospital emergency departments and urgent care centers are sources of sporadic problem-focused care. Surgicenters are examples of specialty clinics. Hospice services for the terminally ill who are expected to live six months or less are most commonly subsidized by charities and government. Prenatal, family planning, and dysplasia clinics are government-funded obstetric and gynecologic specialty clinics respectively, and are usually staffed by nurse practitioners.
Physicians (M.D. and D.O.)
Physicians in the U.S. include those trained by the U.S. medical education system, and those that are international medical graduates who have progressed through the necessary steps to acquire a medical license to practice in a state.
The American College of Physicians, uses the term physician to describe all medical practitioners holding a professional medical degree. In the U.S., however, most physicians have either an Doctor of Medicine (M.D.) or a Doctor of Osteopathic Medicine (D.O.) degree. The American Medical Association as well as the American Osteopathic Association both currently use the term physician to describe members.
Medical products, research and development
As in most other countries, the manufacture and production of pharmaceuticals and medical devices is carried out by private companies. The research and development of medical devices and pharmaceuticals is supported by both public and private sources of funding. In 2003, research and development expenditures were approximately $95 billion with $40 billion coming from public sources and $55 billion coming from private sources. These investments into medical research have made the United States the leader in medical innovation, measured either in terms of revenue or the number of new drugs and devices introduced. In 2006, the United States accounted for three quarters of the world's biotechnology revenues and 82% of world R&D spending in biotechnology. According to multiple international pharmaceutical trade groups, the high cost of patented drugs in the U.S. has encouraged substantial reinvestment in such research and development. Though PPACA, also known as Obamacare or ACA, will force industry to sell medicine at a cheaper price. Reference behind paywall Due to this, it is possible budget cuts will be made on research and development of human health and medicine in America. Reference behind paywall
Healthcare provider employment in the United States
A large demographic shift in the United States is putting pressure on the medical system, and the industries that support it. Roughly 10,000 baby boomers retire every day in the United States which removes many talented and experienced workers from the medical field each year. The demographic shift to an older population is projected to increase medical spending in North America by at least 5%, creating a funding crunch that the government (through medicare and other social services), insurance companies, and individual savings accounts are straining to absorb. Finally, the older population is rapidly increasing demand for healthcare services despite the tight budgets and reduced workforce. All of these factors put pressure on wages and working conditions, with the majority of healthcare jobs seeing salary reductions between 2009 and 2011.
The challenging demographic pressures on the United States' medical system means that more reductions (and imbalances) in wages are coming. Employment opportunities are increasing but job security and employee confidence have both fallen for medical professionals. Highly trained doctors, surgeons, and support staff such as anesthesiologists are insulated from falling wages thanks to high barriers of entry. For staff with less training, formerly well paying jobs are being outsourced or cut to make up budget shortfalls. Additionally, some of the fastest growing health sectors (such as seniors home care) are also some of the lowest paid which could cause supply shortages in the near future.
Spending
Aggregate U.S. hospital costs were $387.3 billion in 2011â€"a 63% increase since 1997 (inflation adjusted). Costs per stay increased 47% since 1997, averaging $10,000 in 2011.
According to the World Health Organization (WHO), total health care spending in the U.S. was 17.9% of its GDP in 2011, the highest in the world. The Health and Human Services Department expects that the health share of GDP will continue its historical upward trend, reaching 19.5% of GDP by 2017. Of each dollar spent on health care in the United States, 31% goes to hospital care, 21% goes to physician/clinical services, 10% to pharmaceuticals, 4% to dental, 6% to nursing homes and 3% to home health care, 3% for other retail products, 3% for government public health activities, 7% to administrative costs, 7% to investment, and 6% to other professional services (physical therapists, optometrists, etc.).
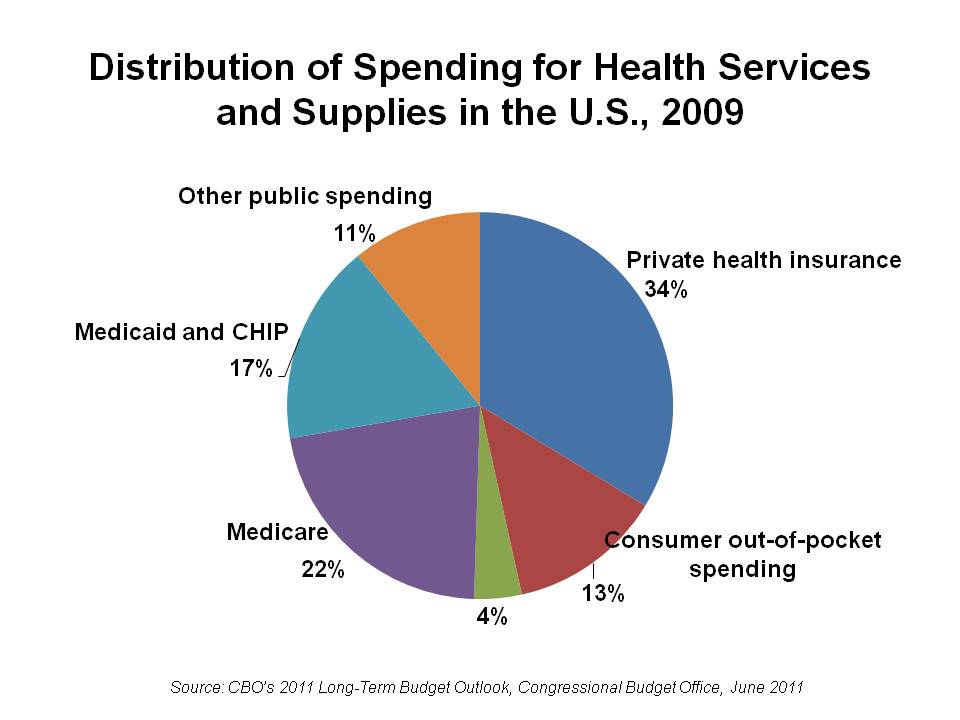
Around 84.7% of Americans have some form of health insurance; either through their employer or the employer of their spouse or parent (59.3%), purchased individually (8.9%), or provided by government programs (27.8%; there is some overlap in these figures). All government health care programs have restricted eligibility, and there is no government health insurance company which covers all Americans. Americans without health insurance coverage in 2007 totaled 15.3% of the population, or 45.7Â million people.
Among those whose employer pays for health insurance, the employee may be required to contribute part of the cost of this insurance, while the employer usually chooses the insurance company and, for large groups, negotiates with the insurance company. Government programs directly cover 27.8% of the population (83Â million), including the elderly, disabled, children, veterans, and some of the poor, and federal law mandates public access to emergency services regardless of ability to pay. Public spending accounts for between 45% and 56.1% of U.S. health care spending.
Some Americans do not qualify for government-provided health insurance, are not provided health insurance by an employer, and are unable to afford, cannot qualify for, or choose not to purchase, private health insurance. When charity or "uncompensated" care is not available, they sometimes simply go without needed medical treatment. This problem has become a source of considerable political controversy on a national level.
Regulation and oversight
Involved organizations and institutions
Healthcare is subject to extensive regulation at both the federal and the state level, much of which "arose haphazardly". Under this system, the federal government cedes primary responsibility to the states under the McCarran-Ferguson Act. Essential regulation includes the licensure of health care providers at the state level and the testing and approval of pharmaceuticals and medical devices by the U.S. Food and Drug Administration (FDA), and laboratory testing. These regulations are designed to protect consumers from ineffective or fraudulent healthcare. Additionally, states regulate the health insurance market and they often have laws which require that health insurance companies cover certain procedures, although state mandates generally do not apply to the self-funded health care plans offered by large employers, which exempt from state laws under preemption clause of the Employee Retirement Income Security Act. In 2010, the Patient Protection and Affordable Care Act (PPACA) was passed by President Barack Obama and includes various new regulations, with one of the most notable being a health insurance mandate which requires all citizens to purchase health insurance. While not regulation per se, the federal government also has a major influence on the healthcare market through its payments to providers under Medicare and Medicaid, which in some cases are used as a reference point in the negotiations between medical providers and insurance companies.
At the federal level, U.S. Department of Health and Human Services oversees the various federal agencies involved in health care. The health agencies are a part of the U.S. Public Health Service, and include the Food and Drug Administration, which certifies the safety of food, effectiveness of drugs and medical products, the Centers for Disease Prevention, which prevents disease, premature death, and disability, the Agency of Health Care Research and Quality, the Agency Toxic Substances and Disease Registry, which regulates hazardous spills of toxic substances, and the National Institutes of Health, which conducts medical research.
State governments maintain state health departments, and local governments (counties and municipalities) often have their own health departments, usually branches of the state health department. Regulations of a state board may have executive and police strength to enforce state health laws. In some states, all members of state boards must be health care professionals. Members of state boards may be assigned by the governor or elected by the state committee. Members of local boards may be elected by the mayor council. The McCarranâ€"Ferguson Act, which cedes regulation to the states, does not itself regulate insurance, nor does it mandate that states regulate insurance. "Acts of Congress" that do not expressly purport to regulate the "business of insurance" will not preempt state laws or regulations that regulate the "business of insurance." The Act also provides that federal anti-trust laws will not apply to the "business of insurance" as long as the state regulates in that area, but federal anti-trust laws will apply in cases of boycott, coercion, and intimidation. By contrast, most other federal laws will not apply to insurance whether the states regulate in that area or not.
Self-policing of providers by providers is a major part of oversight. Many health care organizations also voluntarily submit to inspection and certification by the Joint Commission on Accreditation of Hospital Organizations, JCAHO. Providers also undergo testing to obtain board certification attesting to their skills. A report issued by Public Citizen in April 2008 found that, for the third year in a row, the number of serious disciplinary actions against physicians by state medical boards declined from 2006 to 2007, and called for more oversight of the boards.
The Centers for Medicare and Medicaid Services (CMS) publishes an on-line searchable database of performance data on nursing homes. In 2004, conservative think tank Cato Institute published a study which concluded that regulation provides benefits in the amount of $170Â billion but costs the public up to $340Â billion. The study concluded that the majority of the cost differential arises from medical malpractice, FDA regulations, and facilities regulations.
"Certificates of need" for hospitals
In 1978, the federal government required that all states implement Certificate of Need (CON) programs for cardiac care, meaning that hospitals had to apply and receive certificates prior to implementing the program; the intent was to reduce cost by reducing duplicate investments in facilities. It has been observed that these certificates could be used to increase costs through weakened competition. Many states removed the CON programs after the federal requirement expired in 1986, but some states still have these programs. Empirical research looking at the costs in areas where these programs have been discontinued have not found a clear effect on costs, and the CON programs could decrease costs because of reduced facility construction or increase costs due to reduced competition.
Licensing of providers
The American Medical Association (AMA) has lobbied the government to highly limit physician education since 1910, currently at 100,000 doctors per year, which has led to a shortage of doctors and physicians' wages in the U.S. are double those in the Europe, which is a major reason for the more expensive health care.
An even bigger problem may be that the doctors are paid for procedures instead of results.
The AMA has also aggressively lobbied for many restrictions that require doctors to carry out operations that might be carried out by cheaper workforce. For example, in 1995, 36 states banned or restricted midwifery even though it delivers equally safe care to that by doctors, according to studies . The regulation lobbied by the AMA has decreased the amount and quality of health care, according to the consensus of economist: the restrictions do not add to quality, they decrease the supply of care. Moreover, psychologists, nurses and pharmacists are not allowed to prescribe medicines. Previously nurses were not even allowed to vaccinate the patients without direct supervision by doctors.
36 states require that health care workers undergo criminal background checks.
Emergency Medical Treatment and Active Labor Act (EMTALA)
EMTALA, enacted by the federal government in 1986, requires that hospital emergency departments treat emergency conditions of all patients regardless of their ability to pay and is considered a critical element in the "safety net" for the uninsured, but established no direct payment mechanism for such care. Indirect payments and reimbursements through federal and state government programs have never fully compensated public and private hospitals for the full cost of care mandated by EMTALA. More than half of all emergency care in the U.S. now goes uncompensated. According to some analyses, EMTALA is an unfunded mandate that has contributed to financial pressures on hospitals in the last 20 years, causing them to consolidate and close facilities, and contributing to emergency room overcrowding. According to the Institute of Medicine, between 1993 and 2003, emergency room visits in the U.S. grew by 26%, while in the same period, the number of emergency departments declined by 425.
Mentally ill patients present a unique challenge for emergency departments and hospitals. In accordance with EMTALA, mentally ill patients who enter emergency rooms are evaluated for emergency medical conditions. Once mentally ill patients are medically stable, regional mental health agencies are contacted to evaluate them. Patients are evaluated as to whether they are a danger to themselves or others. Those meeting this criterion are admitted to a mental health facility to be further evaluated by a psychiatrist. Typically, mentally ill patients can be held for up to 72 hours, after which a court order is required.
Quality assurance
Health care quality assurance consists of the "activities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps."
One innovation in encouraging quality of health care is the public reporting of the performance of hospitals, health professionals or providers, and healthcare organizations. However, there is "no consistent evidence that the public release of performance data changes consumer behaviour or improves care."
Overall system effectiveness
Measures of effectiveness
The US health care delivery system unevenly provides medical care of varying quality to its population. In a highly effective health care system, individuals would receive reliable care that meets their needs and is based on the best scientific knowledge available. In order to monitor and evaluate system effectiveness, researchers and policy makers track system measures and trends over time. The US Department of Health and Human Services(HHS) populates a publicly available dashboard called, the Health System Measurement Project (healthmeasures.aspe.hhs.gov), to ensure a robust monitoring system. The dashboard captures the access, quality and cost of care; overall population health; and health system dynamics (e.g., workforce, innovation, health information technology). Included measures align with other system performance measuring activities including the HHS Strategic Plan, the Government Performance and Results Act, Healthy People 2020, and the National Strategies for Quality and Prevention.
Access to care: Cost, affordability, coverage
The US health system does not provide health care to the country's entire population. Individuals acquire health insurance to offset health care spending. However, lack of adequate health insurance persists and is a known barrier to accessing the healthcare system and receiving appropriate and timely care. Measures of accessibility and affordability tracked by national health surveys include: having a usual source of medical care, visiting the dentist yearly, rates of preventable hospitalizations, reported difficulty seeing a specialist, delaying care due to cost, and rates of health insurance coverage.
- As a country, rising health care costs have raised concerns among the public and private sector alike. Between 2000 and 2011, health care expenditures nearly doubled, growing from $1.2 trillion to $2.3 trillion [CDC Health, United States, 2013]. Evidence suggests the rate of growth has slowed in recent years. Other measures of cost captured by national surveys include: health insurance premiums, high out of pocket costs (e.g., deductibles, copayments), and national health expenditures including individual, employer, and government expenditures.
Population health: Quality, prevention, vulnerable populations
The health of the population is also viewed as a measure of the overall effectiveness of the healthcare system. The extent to which the population lives longer healthier lives signals an effective system.
- While life expectancy is one measure, HHS uses a composite health measure that estimates not only the average length of life, but also, the part of life expectancy that is expected to be "in good or better health, as well as free of activity limitations." Between 1997 and 2010, the number of expected high quality life years increased from 61.1 to 63.2 years for newborns.
- The underutilization of preventative measures, rates of preventable illness and prevalence of chronic disease suggest that the US healthcare system does not sufficiently promote wellness. Over the past decade rates of teen pregnancy and low birth rates have come down significantly, but not disappeared. Rates of obesity, heart disease (high blood pressure, controlled high cholesterol), and diabetes are areas of major concern. While chronic disease and multiple co-morbidities became increasingly common among a population of elderly Americans who were living longer, the public health system has also found itself fending off a rise of chronically ill younger generation. According to the US Surgeon General "The prevalence of obesity in the U.S. more than doubled (from 15% to 34%) among adults and more than tripled (from 5% to 17%) among children and adolescents from 1980 to 2008."
- A concern for the health system is that the health gains do not accrue equally to the entire population. In the United States, disparities in health care and health outcomes are widespread. Minorities are more likely to suffer from serious illnesses (e.g., diabetes, heart disease and colon cancer) and less likely to have access to quality health care, including preventative services. Efforts are underway to close the gap and to provide a more equitable system of care.
Innovation: Workforce, healthcare IT, R&D
Finally, the United States tracks investment in the healthcare system in terms of a skilled healthcare workforce, meaningful use of healthcare IT, and R&D output. This aspect of the healthcare system performance dashboard is important to consider when evaluating cost of care in America. That is because in much of the policy debate around the high cost of US healthcare, proponents of highly specialized and cutting edge technologies point to innovation as a marker of an effective health care system.
Compared to other countries
A 2014 study by the private American foundation The Commonwealth Fund found that although the U.S. health care system is the most expensive in the world, it ranks last on most dimensions of performance when compared with Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland and the United Kingdom. The study found that the United States failed to achieve better outcomes than other countries, and is last or near last in terms of access, efficiency and equity. Study date came from international surveys of patients and primary care physicians, as well as information on health care outcomes from The Commonwealth Fund, the World Health Organization, and the Organization for Economic Cooperation and Development.
The U.S. stands 50th in the world with a life expectancy of 78.49. The CIA World Factbook ranked the United States 174th worst (out of 222) â€" meaning 48th best â€" in the world for infant mortality rate (5.98/1,000 live births).
A study found that between 1997 and 2003, preventable deaths declined more slowly in the United States than in 18 other industrialized nations. A 2008 study found that 101,000 people a year die in the U.S. that would not if the health care system were as effective as that of France, Japan, or Australia.
The Organisation for Economic Co-operation and Development (OECD) found that the U.S. ranked poorly in terms of years of potential life lost (YPLL), a statistical measure of years of life lost under the age of 70 that were amenable to being saved by health care. Among OECD nations for which data are available, the United States ranked third last for the health care of women (after Mexico and Hungary) and fifth last for men (Slovakia and Poland also ranked worse).
Recent studies find growing gaps in life expectancy based on income and geography. In 2008, a government-sponsored study found that life expectancy declined from 1983 to 1999 for women in 180 counties, and for men in 11 counties, with most of the life expectancy declines occurring in the Deep South, Appalachia, along the Mississippi River, in the Southern Plains and in Texas. The difference is as high as three years for men, six years for women. The gap is growing between rich and poor and by educational level, but narrowing between men and women and by race. Another study found that the mortality gap between the well-educated and the poorly educated widened significantly between 1993 and 2001 for adults ages 25 through 64; the authors speculated that risk factors such as smoking, obesity and high blood pressure may lie behind these disparities. In 2011 the U.S. National Research Council forecasted that deaths attributed to smoking, on the decline in the US, will drop dramatically, improving life expectancy; it also suggested that one-fifth to one-third of the life expectancy difference can be attributed to obesity which is the worst in the world and has been increasing. In an analysis of breast cancer, colorectal cancer, and prostate cancer diagnosed during 1990â€"1994 in 31 countries, the U.S. had the highest five-year relative survival rate for breast cancer and prostate cancer, although survival was systematically and substantially lower in black U.S. men and women.
The debate about U.S. health care concerns questions of access, efficiency, and quality purchased by the high sums spent. The World Health Organization (WHO) in 2000 ranked the U.S. health care system first in responsiveness, but 37th in overall performance and 72nd by overall level of health (among 191 member nations included in the study). The WHO study has been criticized by the free market advocate David Gratzer because "fairness in financial contribution" was used as an assessment factor, marking down countries with high per-capita private or fee-paying health treatment. The WHO study has been criticized, in an article published in Health Affairs, for its failure to include the satisfaction ratings of the general public. The study found that there was little correlation between the WHO rankings for health systems and the stated satisfaction of citizens using those systems. Countries such as Italy and Spain, which were given the highest ratings by WHO were ranked poorly by their citizens while other countries, such as Denmark and Finland, were given low scores by WHO but had the highest percentages of citizens reporting satisfaction with their health care systems. WHO staff, however, say that the WHO analysis does reflect system "responsiveness" and argue that this is a superior measure to consumer satisfaction, which is influenced by expectations. Furthermore, the relationship between patient satisfaction and health care utilization, expenditures, and outcomes is complex and not well defined.
A report released in April 2008 by the Foundation for Child Development, which studied the period from 1994 through 2006, found mixed results for the health of children in the U.S. Mortality rates for children ages 1 through 4 dropped by a third, and the percentage of children with elevated blood lead levels dropped by 84%. The percentage of mothers who smoked during pregnancy also declined. On the other hand, both obesity and the percentage of low-birth weight babies increased. The authors note that the increase in babies born with low birth weights can be attributed to women delaying childbearing and the increased use of fertility drugs.
In a sample of 13 developed countries the USA was third in its population weighted usage of medication in 14 classes in both 2009 and 2013. The drugs studied were selected on the basis that the conditions treated had high incidence, prevalence and/or mortality, caused significant long-term morbidity and incurred high levels of expenditure and significant developments in prevention or treatment had been made in the last 10 years. The study noted considerable difficulties in cross border comparison of medication use.
System efficiency and equity
Variations in the efficiency of health care delivery can cause variations in outcomes. The Dartmouth Atlas Project, for instance, reported that, for over 20 years, marked variations in how medical resources are distributed and used in the United States were accompanied by marked variations in outcomes. The willingness of physicians to work in an area varies with the income of the area and the amenities it offers, a situation aggravated by a general shortage of doctors in the United States, particularly those who offer primary care. The Affordable Care Act, if implemented, will produce an additional demand for services which the existing stable of primary care doctors will be unable to fill, particularly in economically depressed areas. Training additional physicians would require some years.
Lean manufacturing techniques such as value stream mapping can help identify and subsequently mitigate waste associated with costs of healthcare. Other product engineering tools such as FMEA and Fish Bone Diagrams have been used to improve efficiencies in healthcare delivery.
Efficiency
Preventable deaths
In 2010, coronary artery disease, lung cancer, stroke, chronic obstructive pulmonary diseases, and traffic accidents caused the most years of life lost in the US. Low back pain, depression, musculoskeletal disorders, neck pain, and anxiety caused the most years lost to disability. The most deleterious risk factors were poor diet, tobacco smoking, obesity, high blood pressure, high blood sugar, physical inactivity, and alcohol use. Alzheimer's disease, drug abuse, kidney disease and cancer, and falls caused the most additional years of life lost over their age-adjusted 1990 per-capita rates.
Between 1990 and 2010, among the 34 countries in the OECD, the US dropped from 18th to 27th in age-standardized death rate. The US dropped from 23rd to 28th for age-standardized years of life lost. It dropped from 20th to 27th in life expectancy at birth. It dropped from 14th to 26th for healthy life expectancy.
According to a 2009 study conducted at Harvard Medical School by co-founders of Physicians for a National Health Program, a pro-single payer lobbying group, and published by the American Journal of Public Health, lack of health coverage is associated with nearly 45,000 excess preventable deaths annually. Since then, as the number of uninsured has risen from about 46 million in 2009 to 48.6 million in 2012, the number of preventable deaths due to lack of insurance has grown to about 48,000 per year. The group's methodology has been criticized by economist John C. Goodman for not looking at cause of death or tracking insurance status changes over time, including the time of death.
A 2009 study by former Clinton policy adviser Richard Kronick published in the journal Health Services Research found no increased mortality from being uninsured after certain risk factors were controlled for.
Value for money
A study of international health care spending levels published in the health policy journal Health Affairs in the year 2000 found that the United States spends substantially more on health care than any other country in the Organization for Economic Co-operation and Development (OECD), and that the use of health care services in the U.S. is below the OECD median by most measures. The authors of the study conclude that the prices paid for health care services are much higher in the U.S. than elsewhere. While the 19 next most wealthy countries by GDP all pay less than half what the U.S. does for health care, they have all gained about six years of life expectancy more than the U.S. since 1970.
Delays in seeking care and increased use of emergency care
Uninsured Americans are less likely to have regular health care and use preventive services. They are more likely to delay seeking care, resulting in more medical crises, which are more expensive than ongoing treatment for such conditions as diabetes and high blood pressure. A 2007 study published in JAMA concluded that uninsured people were less likely than the insured to receive any medical care after an accidental injury or the onset of a new chronic condition. The uninsured with an injury were also twice as likely as those with insurance to have received none of the recommended follow-up care, and a similar pattern held for those with a new chronic condition. Uninsured patients are twice as likely to visit hospital emergency rooms as those with insurance; burdening a system meant for true emergencies with less-urgent care needs.
In 2008 researchers with the American Cancer Society found that individuals who lacked private insurance (including those covered by Medicaid) were more likely to be diagnosed with late-stage cancer than those who had such insurance.
The costs of treating the uninsured must often be absorbed by providers as charity care, passed on to the insured via cost shifting and higher health insurance premiums, or paid by taxpayers through higher taxes. However, hospitals and other providers are reimbursed for the cost of providing uncompensated care via a federal matching fund program. Each state enacts legislation governing the reimbursement of funds to providers. In Missouri, for example, providers assessments totaling $800 million are matched â€" $2 for each assessed $1 â€" to create a pool of approximately $2 billion. By federal law these funds are transferred to the Missouri Hospital Association for disbursement to hospitals for the costs incurred providing uncompenstated care including Disproportionate Share Payments (to hospitals with high quantities of uninsured patients), Medicaid shortfalls, Medicaid managed care payments to insurance companies and other costs incurred by hospitals. In New Hampshire, by statute, reimbursable uncompensated care costs shall include: charity care costs, any portion of Medicaid patient care costs that are unreimbursed by Medicaid payments, and any portion of bad debt costs that the commissioner determines would meet the criteria under 42 U.S.C. section 1396r-4(g) governing hospital-specific limits on disproportionate share hospital payments under Title XIX of the Social Security Act.
A report published by the Kaiser Family Foundation in April 2008 found that economic downturns place a significant strain on state Medicaid and SCHIP programs. The authors estimated that a 1%Â increase in the unemployment rate would increase Medicaid and SCHIP enrollment by 1Â million, and increase the number uninsured by 1.1Â million. State spending on Medicaid and SCHIP would increase by $1.4Â billion (total spending on these programs would increase by $3.4Â billion). This increased spending would occur at the same time state government revenues were declining. During the last downturn, the Jobs and Growth Tax Relief Reconciliation Act of 2003 (JGTRRA) included federal assistance to states, which helped states avoid tightening their Medicaid and SCHIP eligibility rules. The authors conclude that Congress should consider similar relief for the current economic downturn.
Variations in provider practices
The treatment given to a patient can vary significantly depending on which health care providers they use. Research suggests that some cost-effective treatments are not used as often as they should be, while overutilization occurs with other health care services. Unnecessary treatments increase costs and can cause patients unnecessary anxiety. The use of prescription drugs varies significantly by geographic region. The overuse of medical benefits is known as moral hazard â€" individuals who are insured are then more inclined to consume health care. The way the Health care system tries to eliminate this problem is through cost sharing tactics like co-pays and deductibles. If patients face more of the economic burden they will then only consume health care when it is necessary. According to the RAND health insurance experiment, individuals with higher Coinsurance rates consumed less health care than those with lower rates. The experiment concluded that with less consumption of care there was generally no loss in societal welfare but, for the poorer and sicker groups of people there were definitely negative effects. These patients were forced to forgo necessary preventative care measures in order to save money leading to late diagnosis of easily treated diseases and more expensive procedures later. With less preventative care, the patient is hurt financially with an increase in expensive visits to the ER.The Health Care costs in the U.S will also rise with these procedures as well. More expensive procedures lead to greater costs.
One study has found significant geographic variations in Medicare spending for patients in the last two years of life. These spending levels are associated with the amount of hospital capacity available in each area. Higher spending did not result in patients living longer.
Care coordination
Primary care doctors are often the point of entry for most patients needing care, but in the fragmented health care system of the U.S., many patients and their providers experience problems with care coordination. For example, a Harris Interactive survey of California physicians found that:
- Four of every ten physicians report that their patients have had problems with coordination of their care in the last 12 months.
- More than 60% of doctors report that their patients "sometimes" or "often" experience long wait times for diagnostic tests.
- Some 20% of doctors report having their patients repeat tests because of an inability to locate the results during a scheduled visit.
According to an article in The New York Times, the relationship between doctors and patients is deteriorating. A study from Johns Hopkins University found that roughly one in four patients believe their doctors have exposed them to unnecessary risks, and anecdotal evidence such as self-help books and web postings suggest increasing patient frustration. Possible factors behind the deteriorating doctor/patient relationship include the current system for training physicians and differences in how doctors and patients view the practice of medicine. Doctors may focus on diagnosis and treatment, while patients may be more interested in wellness and being listened to by their doctors.
Many primary care physicians no longer see their patients while they are in the hospital. Instead, hospitalists are used, which fragments care because hospitalists usually have had no previous relationship with the patient they are treating and do not have a personal knowledge of the patient's medical history. The use of hospitalists is sometimes mandated by health insurance companies as a cost-saving measure which is resented by some primary care physicians.
Administrative costs
The health care system in the U.S. has a vast number of players. There are hundreds, if not thousands, of insurance companies in the U.S. This system has considerable administrative overhead, far greater than in nationalized, single-payer systems, such as Canada's. An oft-cited study by Harvard Medical School and the Canadian Institute for Health Information determined that some 31% of U.S. health care dollars, or more than $1,000 per person per year, went to health care administrative costs, nearly double the administrative overhead in Canada, on a percentage basis.
According to the insurance industry group America's Health Insurance Plans, administrative costs for private health insurance plans have averaged approximately 12% of premiums over the last 40 years. There has been a shift in the type and distribution of administrative expenses over that period. The cost of adjudicating claims has fallen, while insurers are spending more on other administrative activities, such as medical management, nurse help lines, and negotiating discounted fees with health care providers.
A 2003 study published by the Blue Cross and Blue Shield Association (BCBSA) also found that health insurer administrative costs were approximately 11% to 12% of premiums, with Blue Cross and Blue Shield plans reporting slightly lower administrative costs, on average, than commercial insurers. For the period 1998 through 2003, average insurer administrative costs declined from 12.9% to 11.6% of premiums. The largest increases in administrative costs were in customer service and information technology, and the largest decreases were in provider services and contracting and in general administration. The McKinsey Global Institute estimated that excess spending on "health administration and insurance" accounted for as much as 21% of the estimated total excess spending ($477Â billion in 2003).
According to a report published by the CBO in 2008, administrative costs for private insurance represent approximately 12% of premiums. Variations in administrative costs between private plans are largely attributable to economies of scale. Coverage for large employers has the lowest administrative costs. The percentage of premium attributable to administration increases for smaller firms, and is highest for individually purchased coverage. A 2009 study published by BCBSA found that the average administrative expense cost for all commercial health insurance products was represented 9.18% of premiums in 2008. Administrative costs were 11.12% of premiums for small group products and 16.35% in the individual market.
One study of the billing and insurance-related (BIR) costs borne not only by insurers but also by physicians and hospitals found that BIR among insurers, physicians, and hospitals in California represented 20â€"22% of privately insured spending in California acute care settings.
Third-party payment problem and consumer-driven insurance
Most Americans pay for medical services largely through insurance, and this can distort the incentives of consumers since the consumer pays only a portion of the ultimate cost directly. The lack of price information on medical services can also distort incentives. The insurance which pays on behalf of insureds negotiate with medical providers, sometimes using government-established prices such as Medicaid billing rates as a reference point. This reasoning has led for calls to reform the insurance system to create a consumer-driven health care system whereby consumers pay more out-of-pocket. In 2003, the Medicare Prescription Drug, Improvement, and Modernization Act was passed, which encourages consumers to have a high-deductible health plan and a health savings account.
Overall costs
The U.S. spends more as a percentage of GDP than similar countries, and this can be explained either through higher prices for services themselves, higher costs to administer the system, or more utilization of these services, or to a combination of these elements.
Free-market advocates claim that the health care system is "dysfunctional" because the system of third-party payments from insurers removes the patient as a major participant in the financial and medical choices that affect costs. The Cato Institute claims that because government intervention has expanded insurance availability through programs such as Medicare and Medicaid, this has exacerbated the problem. According to a study paid for by America's Health Insurance Plans (a Washington lobbyist for the health insurance industry) and carried out by PriceWaterhouseCoopers, increased utilization is the primary driver of rising health care costs in the U.S. The study cites numerous causes of increased utilization, including rising consumer demand, new treatments, more intensive diagnostic testing, lifestyle factors, the movement to broader-access plans, and higher-priced technologies. The study also mentions cost-shifting from government programs to private payers. Low reimbursement rates for Medicare and Medicaid have increased cost-shifting pressures on hospitals and doctors, who charge higher rates for the same services to private payers, which eventually affects health insurance rates.
Health care costs rising far faster than inflation have been a major driver for health care reform in the United States. Surgical, injury, and maternal and neonatal health hospital visit costs increased by more than 2% each year from 2003-2011. Further, while average hospital discharges remained stable, hospital costs rost from $9,100 in 2003 to $10,600 in 2011, and were projected to be $11,000 by 2013.
In March 2010, Massachusetts released a report on the cost drivers which it called "unique in the nation". The report noted that providers and insurers negotiate privately, and therefore the prices can vary between providers and insurers for the same services, and it found that the variation in prices did not vary based on quality of care but rather on market leverage; the report also found that price increases rather than increased utilization explained the spending increases in the past several years.
Equity
Coverage
Enrollment rules in private and governmental programs result in millions of Americans going without health care coverage, including children. The U.S. Census Bureau estimated that 45.7Â million Americans (15.3% of the total population) had no health insurance coverage in 2007. However, statistics regarding the insured population are difficult to pinpoint for a number of factors, with the Census Bureau writing that "health insurance coverage is likely to be underreported". Further, such statistics do not provide insight into the reason a given person might be uninsured. Studies have shown that approximately one third of this 45.7 million person population of uninsured persons is actually eligible for government insurance programmes such as Medicaid/Medicare, but has elected not to enroll. The largest proportion of the population of uninsured Americans is persons earning in excess of $50,000 per annum, with those earning over $75,000 p.a. comprising the fastest-growing segment of the uninsured population. U.S. Citizens who earn too much money to qualify for government assistance with insurance programs but who do not earn enough to purchase a private health insurance plan make up approximately 2.7% percent of the total US population (8.2 million of approximately 300 million total population, by 2003 figures).
States like California offer insurance coverage for children of low income families, but not for adults; other states do not offer such coverage at all: both parent and child are caught in the notorious coverage "gap." Although EMTALA certainly keeps alive many working-class people who are badly injured, the 1986 law neither requires the provision of preventive or rehabilitative care, nor subsidizes such care, and it does nothing about the difficulties in the American mental health system.
Coverage gaps also occur among the insured population. Johns Hopkins University professor Vicente Navarro stated in 2003, "the problem does not end here, with the uninsured. An even larger problem is the underinsured" and "The most credible estimate of the number of people in the United States who have died because of lack of medical care was provided by a study carried out by Harvard Medical School Professors Himmelstein and Woolhandler. They concluded that almost 100,000 people died in the U.S. yearly because of lack of needed care." Another study by the Commonwealth Fund published in Health Affairs estimated that 16 million U.S. adults were underinsured in 2003. The study defined underinsurance as characterized by at least one of the following conditions: annual out-of-pocket medical expenses totaling 10% or more of income, or 5% or more among adults with incomes below 200% of the federal poverty level; or health plan deductibles equaling or exceeding 5% of income. The underinsured were significantly more likely than those with adequate insurance to forgo health care, report financial stress because of medical bills, and experience coverage gaps for such items as prescription drugs. The study found that underinsurance disproportionately affects those with lower incomes â€" 73% of the underinsured in the study population had annual incomes below 200% of the federal poverty level. Another study focusing on the effect of being uninsured found that individuals with private insurance were less likely to be diagnosed with late-stage cancer than either the uninsured or Medicaid beneficiaries. A study examining the effects of health insurance cost-sharing more generally found that chronically ill patients with higher co-payments sought less care for both minor and serious symptoms while no effect on self-reported health status was observed. The authors concluded that the effect of cost sharing should be carefully monitored.
Coverage gaps and affordability also surfaced in a 2007 international comparison by the Commonwealth Fund. Among adults surveyed in the U.S., 37% reported that they had foregone needed medical care in the previous year because of cost; either skipping medications, avoiding seeing a doctor when sick, or avoiding other recommended care. The rate was higher â€" 42% â€" among those with chronic conditions. The study reported that these rates were well above those found in the other six countries surveyed: Australia, Canada, Germany, the Netherlands, New Zealand, and the UK. The study also found that 19% of U.S. adults surveyed reported serious problems paying medical bills, more than double the rate in the next highest country.
Mental health
A lack of mental health coverage for Americans bears significant ramifications to the U.S. economy and social system. A report by the U.S. Surgeon General found that mental illnesses are the second leading cause of disability in the nation and affect 20% of all Americans. It is estimated that less than half of all people with mental illnesses receive treatment (or specifically, an ongoing, much needed, and managed care; where medication alone, cannot easily remove mental conditions) due to factors such as stigma and lack of access to care.
The Paul Wellstone Mental Health and Addiction Equity Act of 2008 mandates that group health plans provide mental health and substance-related disorder benefits that are at least equivalent to benefits offered for medical and surgical procedures. The legislation renews and expands provisions of the Mental Health Parity Act of 1996. The law requires financial equity for annual and lifetime mental health benefits, and compels parity in treatment limits and expands all equity provisions to addiction services. Insurance companies and third-party disability administrators (most notably, Sedgwick CMS) used loopholes and, though providing financial equity, they often worked around the law by applying unequal co-payments or setting limits on the number of days spent in inpatient or outpatient treatment facilities.
Medical underwriting and the uninsurable
In most states in the U.S., people seeking to purchase health insurance directly must undergo medical underwriting. Insurance companies seeking to mitigate the problem of adverse selection and manage their risk pools screen applicants for pre-existing conditions. Insurers reject many applicants or quote increased rates for those with pre-existing conditions. Diseases that can make an individual uninsurable include serious conditions, such as arthritis, cancer, and heart disease, but also such common ailments as acne, being 20Â pounds over or under weight, and old sports injuries. An estimated 5Â million of those without health insurance are considered "uninsurable" because of pre-existing conditions.
Proponents of medical underwriting argue that it ensures that individual health insurance premiums are kept as low as possible. Critics of medical underwriting believe that it unfairly prevents people with relatively minor and treatable pre-existing conditions from obtaining health insurance.
One large industry survey found that 13% of applicants for individual health insurance who went through medical underwriting were denied coverage in 2004. Declination rates increased significantly with age, rising from 5% for those under 18 to just under one-third for those aged 60 to 64. Among those who were offered coverage, the study found that 76% received offers at standard premium rates, and 22% were offered higher rates. The frequency of increased premiums also increased with age, so for applicants over 40, roughly half were affected by medical underwriting, either in the form of denial or increased premiums. In contrast, almost 90% of applicants in their 20s were offered coverage, and three-quarters of those were offered standard rates. Seventy percent of applicants age 60â€"64 were offered coverage, but almost half the time (40%) it was at an increased premium. The study did not address how many applicants who were offered coverage at increased rates chose to decline the policy. A study conducted by the Commonwealth Fund in 2001 found that, among those aged 19 to 64 who sought individual health insurance during the previous three years, the majority found it unaffordable, and less than a third ended up purchasing insurance. This study did not distinguish between consumers who were quoted increased rates due to medical underwriting and those who qualified for standard or preferred premiums. Some states have outlawed medical underwriting as a prerequisite for individually purchased health coverage. These states tend to have the highest premiums for individual health insurance.
Demographic differences
Health disparities are well documented in the U.S. in ethnic minorities such as African Americans, Native Americans, and Hispanics. When compared to whites, these minority groups have higher incidence of chronic diseases, higher mortality, and poorer health outcomes. Among the disease-specific examples of racial and ethnic disparities in the United States is the cancer incidence rate among African Americans, which is 25% higher than among whites. In addition, adult African Americans and Hispanics have approximately twice the risk as whites of developing diabetes and have higher overall obesity rates. Minorities also have higher rates of cardiovascular disease and HIV/AIDS than whites. Caucasian Americans have much lower life expectancy than Asian Americans. A 2001 study found large racial differences exist in healthy life expectancy at lower levels of education.
Public spending is highly correlated with age; average per capita public spending for seniors was more than five times that for children ($6,921 versus $1,225). Average public spending for non-Hispanic blacks ($2,973) was slightly higher than that for whites ($2,675), while spending for Hispanics ($1,967) was significantly lower than the population average ($2,612). Total public spending is also strongly correlated with self-reported health status ($13,770 for those reporting "poor" health versus $1,279 for those reporting "excellent" health). Seniors comprise 13% of the population but take 1/3 of all prescription drugs. The average senior fills 38 prescriptions annually. A new study has also found that older men and women in the South are more often prescribed antibiotics than older Americans elsewhere, even though there is no evidence that the South has higher rates of diseases requiring antibiotics.
There is considerable research into inequalities in health care. In some cases these inequalities are caused by income disparities that result in lack of health insurance and other barriers to receiving services. According to the 2009 National Healthcare Disparities Report, uninsured Americans are less likely to receive preventive services in health care. For example, minorities are not regularly screened for colon cancer and the death rate for colon cancer has increased among African Americans and Hispanic people. In other cases, inequalities in health care reflect a systemic bias in the way medical procedures and treatments are prescribed for different ethnic groups. Raj Bhopal writes that the history of racism in science and medicine shows that people and institutions behave according to the ethos of their times. Nancy Krieger wrote that racism underlies unexplained inequities in health care, including treatment for heart disease, renal failure, bladder cancer, and pneumonia. Raj Bhopal writes that these inequalities have been documented in numerous studies. The consistent and repeated findings were that black Americans received less health care than white Americans â€" particularly when the care involved expensive new technology. One recent study has found that when minority and white patients use the same hospital, they are given the same standard of care.
Drug efficiency and safety
The Food and Drug Administration (FDA) is the primary institution tasked with the safety and effectiveness of human and veterinary drugs. It also is responsible for making sure drug information is accurately and informatively presented to the public. The FDA reviews and approves products and establishes drug labeling, drug standards, and medical device manufacturing standards. It sets performance standards for radiation and ultrasonic equipment.
One of the more contentious issues related to drug safety is immunity from prosecution. In 2004, the FDA reversed a federal policy, arguing that FDA premarket approval overrides most claims for damages under state law for medical devices. In 2008 this was confirmed by the Supreme Court in Riegel v. Medtronic.
On June 30, 2006, an FDA ruling went into effect extending protection from lawsuits to pharmaceutical manufacturers, even if it was found that they submitted fraudulent clinical trial data to the FDA in their quest for approval. This left consumers who experience serious health consequences from drug use with little recourse. In 2007, the House of Representatives expressed opposition to the FDA ruling, but the Senate took no action. On March 4, 2009, an important U.S. Supreme Court decision was handed down. In Wyeth v. Levine, the court asserted that state-level rights of action could not be pre-empted by federal immunity and could provide "appropriate relief for injured consumers." In June 2009, under the Public Readiness and Emergency Preparedness Act, Secretary of Health and Human Services Kathleen Sebelius signed an order extending protection to vaccine makers and federal officials from prosecution during a declared health emergency related to the administration of the swine flu vaccine.
Impact of drug companies
The U.S. is one of two countries in the world that allows direct-to-consumer advertising of prescription drugs. Critics note that drug advertisements cost money which they believe have raised the overall price of drugs.
When health care legislation was being written in 2009, the drug companies were asked to support the legislation in return for not allowing importation of drugs from foreign countries.
Political issues
Prescription drug prices
During the 1990s, the price of prescription drugs became a major issue in American politics as the prices of many new drugs increased exponentially, and many citizens discovered that neither the government nor their insurer would cover the cost of such drugs. Per capita, the U.S. spends more on pharmaceuticals than any other country. National expenditures on pharmaceuticals accounted for 12.9% of total health care costs, compared to an OECD average of 17.7% (2003 figures). Some 25% of out-of-pocket spending by individuals is for prescription drugs.
The U.S. government has taken the position (through the Office of the United States Trade Representative) that U.S. drug prices are rising because U.S. consumers are effectively subsidizing costs which drug companies cannot recover from consumers in other countries (because many other countries use their bulk-purchasing power to aggressively negotiate drug prices). The U.S. position (consistent with the primary lobbying position of the Pharmaceutical Research and Manufacturers of America) is that the governments of such countries are free riding on the backs of U.S. consumers. Such governments should either deregulate their markets, or raise their domestic taxes in order to fairly compensate U.S. consumers by directly remitting the difference (between what the companies would earn in an open market versus what they are earning now) to drug companies or to the U.S. government. In turn, pharmaceutical companies would be able to continue to produce innovative pharmaceuticals while lowering prices for U.S. consumers. Currently, the U.S., as a purchaser of pharmaceuticals, negotiates some drug prices but is forbidden by law from negotiating drug prices for the Medicare program due to the Medicare Prescription Drug, Improvement, and Modernization Act passed in 2003. Democrats have charged that the purpose of this provision is merely to allow the pharmaceutical industry to profiteer off of the Medicare program.
Debate
A poll released in March 2008 by the Harvard School of Public Health and Harris Interactive found that Americans are divided in their views of the U.S. health system, and that there are significant differences by political affiliation. When asked whether the U.S. has the best health care system or if other countries have better systems, 45% said that the U.S. system was best and 39% said that other countries' systems are better. Belief that the U.S. system is best was highest among Republicans (68%), lower among independents (40%), and lowest among Democrats (32%). Over half of Democrats (56%) said they would be more likely to support a presidential candidate who advocates making the U.S. system more like those of other countries; 37% of independents and 19% of Republicans said they would be more likely to support such a candidate. 45% of Republicans said that they would be less likely to support such a candidate, compared to 17% of independents and 7% of Democrats.
A 2004 Institute of Medicine (IOM) report said, "the United States is among the few industrialized nations in the world that does not guarantee access to health care for its population." There is currently an ongoing political debate centering around questions of access, efficiency, quality, and sustainability. Whether a government-mandated system of universal health care should be implemented in the U.S. remains a hotly debated political topic, with Americans divided along party lines in their views of the U.S. health system and what should be done to improve it. Those in favor of universal health care argue that the large number of uninsured Americans creates direct and hidden costs shared by all, and that extending coverage to all would lower costs and improve quality. Cato Institute Senior Fellow Alan Reynolds argues that people should be free to opt out of health insurance, citing a study by Economists Craig Perry and Harvey Rosen that found "the lack of health insurance among the self-employed does not affect their health. For virtually every subjective and objective measure of their health status, the self-employed and wage-earners are statistically indistinguishable for each other." Both sides of the political spectrum have also looked to more philosophical arguments, debating whether people have a fundamental right to have health care provided to them by their government.
An impediment to implementing any U.S. healthcare reform that does not benefit insurance companies or the private health care industry is the power of insurance company and health care industry lobbyists. Possibly as a consequence of the power of lobbyists, key politicians such as Senator Max Baucus have taken the option of single payer health care off the table entirely. In a June 2009 NBC News/Wall Street Journal survey, 76% said it was either "extremely" or "quite" important to "give people a choice of both a public plan administered by the federal government and a private plan for their health insurance."
Advocates for single-payer health care often point to other countries, where national government-funded systems produce better health outcomes at lower cost. Opponents deride this type of system as "socialized medicine", and it has not been one of the favored reform options by Congress or the President in both the Clinton and Obama reform efforts. It has been pointed out that socialized medicine is a system in which the government owns the means of providing medicine. England is an example of socialized system, as, in America, is the Veterans Health Administration. Medicare is an example of a mostly single-payer system, as is France. Both of these systems have private insurers to choose from, but the government is the dominant purchaser.
As an example of how government intervention has had unintended consequences, in 1973, the federal government passed the Health Maintenance Organization Act, which heavily subsidized the HMO business model â€" a model that was in decline prior to such legislative intervention. The law was intended to create market incentives that would lower health care costs, but HMOs have never achieved their cost-reduction potential.
Piecemeal market-based reform efforts are complex. One study evaluating current popular market-based reform policy packages concluded that if market-oriented reforms are not implemented on a systematic basis with appropriate safeguards, they have the potential to cause more problems than they solve.
According to economist and former U.S. Secretary of Labor, Robert Reich, only a "big, national, public option" can force insurance companies to cooperate, share information, and reduce costs. Scattered, localized, "insurance cooperatives" are too small to do that and are "designed to fail" by the moneyed forces opposing Democratic health care reform. The Patient Protection and Affordable Care Act, signed into law in March 2010, did not include such an option.
Reform
The Patient Protection and Affordable Care Act (Public Law 111-148) is a health care reform bill that was signed into law in the United States by President Barack Obama on March 23, 2010. Along with the Health Care and Education Reconciliation Act of 2010 (passed March 25), the Act is a product of the health care reform agenda of the Democratic 111th Congress and the Obama administration.
The law includes a large number of health-related provisions to take effect over the next four years, including expanding Medicaid eligibility for people making up to 133% of FPL, subsidizing insurance premiums for peoples making up to 400% of FPL ($88,000 for family of 4) so their maximum "out-of-pocket" pay will be from 2% to 9.8% of income for annual premium, providing incentives for businesses to provide health care benefits, prohibiting denial of coverage and denial of claims based on pre-existing conditions, establishing health insurance exchanges, prohibiting insurers from establishing annual spending caps and support for medical research. The costs of these provisions are offset by a variety of taxes, fees, and cost-saving measures, such as new Medicare taxes for high-income brackets, taxes on indoor tanning, cuts to the Medicare Advantage program in favor of traditional Medicare, and fees on medical devices and pharmaceutical companies; there is also a tax penalty for citizens who do not obtain health insurance (unless they are exempt due to low income or other reasons). The Congressional Budget Office estimates that the net effect (including the reconciliation act) will be a reduction in the federal deficit by $143Â billion over the first decade.
In May 2011, the state of Vermont became the first state to pass legislation establishing a Single-Payer health care system. The legislation, known as Act 48, establishes health care in the state as a "human right" and lays the responsibility on the state to provide a health care system which best meets the needs of the citizens of Vermont. The state is currently in the studying phase of how best to implement this system.
Health insurance coverage for immigrants
Of the 26.2 million foreign immigrants living in the US in 1998, 62.9% were non-U.S. citizens. In 1997, 34.3% of non-U.S. citizens living in America did not have health insurance coverage opposed to the 14.2% of native-born Americans who do not have health insurance coverage. Among those immigrants who became citizens, 18.5% were uninsured, as opposed to noncitizens, who are 43.6% uninsured. In each age and income group, immigrants are less likely to have health insurance. With the recent healthcare changes, many legal immigrants with various immigration statuses now are able qualify for affordable health insurance. Options vary according to the immigrants' age and how long they have been permanent residents.
Health insurance coverage for visitors to the U.S.
Visitors to the U.S. cannot purchase health insurance that is available for U.S. citizens and permanent residents. Most domestic insurance policies purchased overseas cease to be effective inside the U.S., when individuals cross their home country borders during international travel. Currently, it is not mandatory for short-term visitors to U.S. to provide proof of travel medical insurance coverage to obtain a legal visa to enter the U.S. However, considering cost of healthcare for the uninsured in the U.S., many foreigners without residence in the U.S., and visiting the U.S. can benefit by buying a visitors health insurance protection plan that covers emergency expenses such as medical evacuation and treatment for sickness or injuries while in the U.S.
About the author
 Admin
Admin
Duis sed tellus et tortor vestibulum gravida. Praesent elementum elit at tellus. Curabitur metus ipsum, luctus eu, malesuada ut, tincidunt sed, diam. Donec quis mi sed magna hendrerit accumsan.
0 comments: